What Is the NAPLEX?
The gateway exam every pharmacy graduate faces
The North American Pharmacist Licensure Examination is the standardized computer-adaptive test administered by the National Association of Boards of Pharmacy (NABP) to evaluate pharmacy graduates' competency and readiness for independent practice. This isn't some optional credential. You need it. Every single state in the U.S., plus the District of Columbia, Puerto Rico, Virgin Islands, and Guam requires passing the NAPLEX for initial pharmacy licensure. There's no way around it if you want to practice.
Think of it as pharmacy's version of the bar exam for lawyers or what the USMLE is for physicians. The exam measures your ability to apply knowledge, skills, and abilities required for safe and effective pharmacist practice in patient-centered care settings. Not just recall facts from school. Actually apply them in real scenarios.
How the computer-adaptive format actually works
Here's where NAPLEX gets interesting. It uses computer-adaptive testing (CAT) format where question difficulty adjusts based on your performance. Answer correctly? Next question gets harder. Miss one? The algorithm backs off a bit. This makes each exam unique, which freaks some people out because you can't compare your experience directly with your classmate who tested the same day, sat in the same testing center, probably ate lunch together beforehand.
The exam consists of 250 multiple-choice questions administered over 6 hours. But here's the catch: only 225 are scored items. The other 25 are pretest items (unscored) that NABP uses to evaluate for future exams. You won't know which is which, so you've gotta treat every question like it counts.
NAPLEX focuses on three major competency areas: patient-centered care, medication safety, and health system management. The exam tests clinical judgment, therapeutic knowledge, pharmaceutical calculations, drug information interpretation, and patient counseling scenarios. It's not asking you to regurgitate the Krebs cycle or memorize every enzyme pathway. It wants to know if you can safely manage a diabetic patient's medication regimen or catch a dangerous drug interaction before it happens.
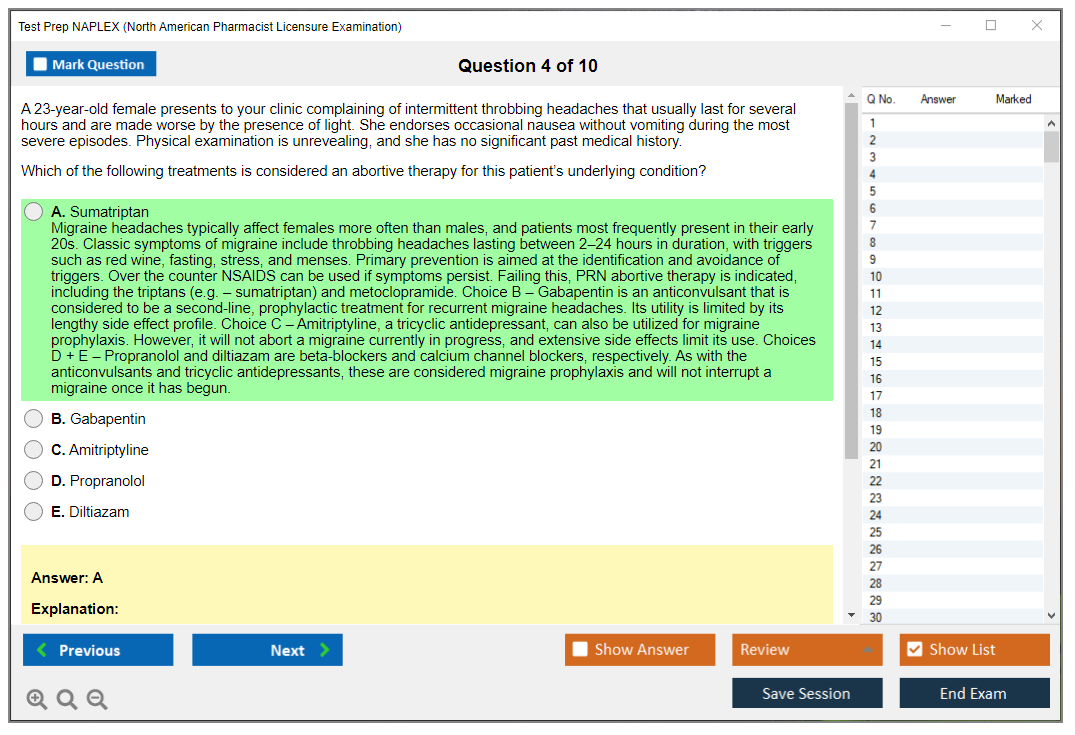
NAPLEX differs from pharmacy school exams by putting the focus on practical application over pure memorization. Your pharmacology professor might've tested you on mechanism of action for 50 beta-blockers. NAPLEX asks which one you'd recommend for a pregnant patient with hypertension who also has asthma. See the difference? Way more clinical.
One more thing about scoring: NAPLEX is criterion-referenced, meaning candidates compete against a standard rather than each other. There's no curve. Your friend passing doesn't make it harder for you to pass, which is pretty refreshing compared to the competitive nightmare of some other standardized tests like the MCAT-Test.
Who takes this thing and when should you schedule it
All pharmacy graduates from ACPE-accredited programs who seek U.S. pharmacy licensure must pass NAPLEX. International pharmacy graduates have an extra hoop. Credentials must be evaluated through FPGEC (Foreign Pharmacy Graduate Examination Committee) before NAPLEX eligibility. That process takes time, so plan ahead if that's your situation.
Timing matters more than most people realize. Optimal timing is within 3-6 months after PharmD graduation when clinical knowledge remains fresh. You just spent four years (that brutal APPE year especially) immersed in this content. Strike while the iron's hot.
Some states allow testing before graduation, typically final semester, while others require diploma verification first. Check your state board requirements early because this varies wildly. Delaware might let you test in April of your graduating year. Pennsylvania might make you wait until your diploma posts in June. The inconsistency is frustrating.
You should coordinate NAPLEX with MPJE (Multistate Pharmacy Jurisprudence Examination) or state-specific law exams for complete licensure. Some people knock them out back-to-back over two days. Others space them two weeks apart. There's no perfect answer. It depends on your test-taking stamina and how much law content you retained from your jurisprudence course, which most people found pretty dry if we're being honest.
Think about APPE completion, job start dates, and state board processing times when you schedule. Got a job offer that starts July 1st? You better pass NAPLEX and get your license application submitted by early May at the absolute latest. State boards can take 4-8 weeks to process everything even after you pass both exams. Seems excessive but that's bureaucracy for you.
Here's something useful: candidates can take NAPLEX in any Pearson VUE testing state regardless of intended licensure state. Live in rural Wyoming but there's a testing center 90 minutes away in Colorado? Take it there. Your scores transfer to whichever state board you're applying through. Pretty convenient.
What about gaps between graduation and testing
Not gonna lie, if you delayed testing years after graduation, you're facing more work. I've seen people who graduated in 2018 and didn't test until 2023 because life happened (family stuff, career pivots, whatever) and they needed 12+ week study plans using full NAPLEX study materials because therapeutic guidelines changed, new drugs launched, and they forgot a ton of content. Can't really blame them.
The NAPLEX exam gets harder when you're rusty. Fresh graduates might review calculations and brush up on weak therapeutic areas. Someone five years out? They basically need to relearn entire disease state management protocols from scratch, which is rough. Kind of like the old pharmacy school joke about remembering which statin is which when they all end in '-vastatin' and your brain just gives up. Similar challenge to how someone preparing for the GRE-Test after years in the workforce faces different hurdles than a current student who's still in academic mode.
Bottom line? Test sooner rather than later if possible. Your future self will thank you when you're not trying to remember the first-line treatment for community-acquired pneumonia while juggling a full-time job and family obligations. Who wants that kind of stress?
NAPLEX Prerequisites and Eligibility
NAPLEX overview (North American Pharmacist Licensure Examination)
The NAPLEX is the North American Pharmacist Licensure Examination. It's huge.
This is your clinical competency checkpoint before you can practice pharmacy anywhere in the U.S., and honestly, it's where everything you've studied comes together. Pharmacotherapy knowledge, patient safety protocols, all those calculation drills. The scenarios feel way less like textbook questions and more like "okay, what would you actually do for this patient right now?"
Here's the thing: people call it Test Prep NAPLEX season for a reason, and it's because everyone's stressed. You're not just memorizing facts from some NAPLEX study guide and praying they stick. You're proving you can actually apply the NAPLEX exam objectives to messy, real-world patient cases. The exam's pretty ruthless about punishing surface-level memorization, especially when dosing decisions, renal function adjustments, drug interactions, and monitoring parameters all collide in one vignette and you've gotta pick the safest move fast.
Who needs the NAPLEX and when to take it
Want a pharmacist license? You need the NAPLEX. Period.
Most candidates sit for it after graduation once their state board gives clearance, but some states let you test early, like right before graduation, if your paperwork's tight and your program's timing cooperates.
Timing matters. Like, a lot. Graduation season absolutely stacks the calendar, and May through August turns into a zoo where Pearson VUE slots vanish before you finish your coffee, so your planning needs to start way earlier than your panic does.
The degree requirement (and what "approved" really means)
The primary prerequisite? Completing a Doctor of Pharmacy (PharmD) degree from an ACPE-accredited college or school of pharmacy. ACPE, that's the Accreditation Council for Pharmacy Education, is the recognized accrediting body for U.S. pharmacy programs, meaning NABP and state boards actually trust ACPE's seal when deciding whether you're allowed to test.
No ACPE accreditation? No normal pathway. That's just reality.
Most states also require full completion of experiential education hours before testing, including IPPEs and APPEs. This trips people up constantly because they assume "I'm basically done" counts, but boards usually want "done done." Meaning your school officially confirms you finished the curriculum requirements, not that you're close and your preceptor thinks you're great.
International graduates and the FPGEC route
International pharmacy graduates typically can't just roll up with their degree and register. They usually must complete the FPGEC certification process through NABP, which includes credential evaluation, passing the FPGEE exam, and meeting English language requirements via TOEFL when applicable. I mean, it's paperwork-heavy and the timelines stretch long, so if you're mapping out North American Pharmacist Licensure Examination prep, build in months, not weeks.
Credential review isn't instant.
TOEFL scheduling isn't either.
Also, your specific state board might pile extra requirements on top of FPGEC, so you've gotta check the board's rules for your state, not just rely on what worked for your friend somewhere else.
Intern registration and experiential hour completion
Some states require candidates to register as pharmacy interns with their state board during school. You can be doing everything right academically and still slam into delays because you forgot some state-level intern registration step back in P2 year. Boards care deeply about documented training hours, and they want that trail squeaky clean.
IPPEs and APPEs matter here again. Most boards expect completion of all experiential hours before approving you to sit, and if you're missing one rotation sign-off or your hours weren't posted correctly, that can stall eligibility even when your NAPLEX study materials are literally sitting ready on your desk.
Newly accredited programs and conditional accreditation situations
Special circumstances happen. The most common?
Graduating from a newly accredited PharmD program or one with candidate or conditional accreditation status during your enrollment. Some states accept those graduates without drama, others want additional verification from the school or ACPE documentation proving the program met standards at your graduation time.
Ask early. Seriously, just ask.
You really don't want to discover an administrative roadblock after you've already paid fees and rearranged your entire life around an exam date. I remember a classmate who assumed everything was fine because her school had gotten full accreditation two months before graduation, but her state board still wanted a formal letter from ACPE explaining the timeline. Cost her an extra month of waiting and way more stress than necessary.
Graduation verification to NABP
You don't just self-attest graduation and move on. Your school must submit official proof, typically an official transcript or graduation certification, directly to NABP. Until NABP receives that, your NAPLEX prerequisites aren't considered satisfied in their system, and you can wind up stuck in limbo even if you're ready to demolish pharmacy licensure exam practice questions all day long.
Applying through the state board first
Here's the order that catches people off guard: you generally apply for licensure through your specific state board of pharmacy first, then the board determines eligibility. After that, approval flows through NABP. Not gonna lie, this is where timelines explode because every board moves at its own glacial pace and some boards are incredibly strict about "complete application" meaning every single box checked, every document received, every fee cleared.
Processing times vary wildly by state. Two to eight weeks is common. And that's gotta happen before your NAPLEX registration goes anywhere useful.
NABP e-Profile setup and registration basics
You'll create an NABP account through their e-Profile system. The steps are straightforward enough: make the account, enter personal information exactly as it appears on your government ID, add education details, select the exam and jurisdiction, track application status. The name matching part's a huge deal because a tiny mismatch can block you at the test center even when everything else is perfect.
Then you wait.
Boards review. State board applications often include background checks, fingerprinting, application fees, sometimes character references. They review your file and decide eligibility before issuing authorization to test. Common disqualifying factors? Felony convictions, previous license revocations, academic integrity violations. And yeah, boards can demand documentation, court records, or lengthy explanations.
You can apply for licensure in multiple states at the same time if you're planning reciprocity or want multiple licenses, but it adds cost and admin chaos, so keep a spreadsheet and don't rely on memory alone.
ATT, ID rules, and scheduling at Pearson VUE
Authorization to Test (ATT) is official permission from the state board transmitted through NABP's system that lets you schedule. ATT validity's typically 90 days from issuance, though some states allow longer windows, and if it expires you might be paying again and restarting steps you really didn't want to repeat.
For ID? Bring a valid, unexpired government-issued ID with photo and signature, and the name must match your NABP registration exactly. No match, no test. It's brutal but predictable, so fix mismatches early.
Once you've got ATT, you schedule with Pearson VUE online, by phone, or through their mobile app. Appointments are available year-round at Pearson VUE centers nationwide, but availability shifts fast around graduation. Schedule two to four weeks ahead for your preferred date and location, especially May through August.
Rescheduling's possible. But you generally must reschedule at least three business days before your appointment or you can forfeit the exam fee entirely, which stings even worse when you remember the NAPLEX exam cost is already painful.
If you need special testing accommodations, you go through NABP's ADA coordinator with documentation. Start that process early because approvals take time and the clock on your ATT window doesn't care about your paperwork stress. Timelines don't pause for admin headaches.
And yeah, while you're juggling all this? Keep studying. Your NAPLEX practice test scores, your grasp of NAPLEX competency statements, your comfort with MPJE vs NAPLEX differences won't fix eligibility problems, but eligibility problems will absolutely block you from testing no matter how prepared you are.
NAPLEX Exam Objectives and Content Outline
Understanding NABP's three core competency areas
The NAPLEX structures everything around three major competency areas developed by the National Association of Boards of Pharmacy. Real-world stuff. These are not random, they reflect what you will actually do as a licensed pharmacist once you are out there dealing with patients who have got medication lists a mile long. Area 1 dominates the exam at roughly 67% of questions, Area 2 takes about 22%, and Area 3 rounds out the remaining 11%. Understanding this breakdown changes how you study because you are not treating everything equally.
The competency statements themselves describe observable behaviors. They are not testing whether you memorized a drug list, they want to see if you can actually solve problems like you would in practice. Questions integrate across therapeutic areas, so you might get a heart failure patient who also has diabetes and renal impairment. That is the real world.
Identifying, analyzing, and solving drug therapy problems makes up two-thirds of your exam
Look, Area 1 is massive. It covers everything from obtaining patient information to designing complete therapeutic plans. You will assess whether current drug therapy is appropriate, effective, and safe for that specific patient. The scenarios get detailed. Age matters, kidney function matters, pregnancy status matters, what other medications they are taking definitely matters.
Questions here test your ability to identify drug interactions before they happen. You need to recognize adverse effects, know contraindications cold, and understand therapeutic monitoring parameters. Like, when do you check a digoxin level versus a vancomycin trough? What labs do you monitor for someone starting an ACE inhibitor?
The subtopics include interpreting patient data (labs, key signs, medication histories), evaluating drug therapy for problems, and then actually designing patient-specific plans. This is where clinical knowledge separates people who pass easily from those who struggle. You cannot just memorize, you have to apply.
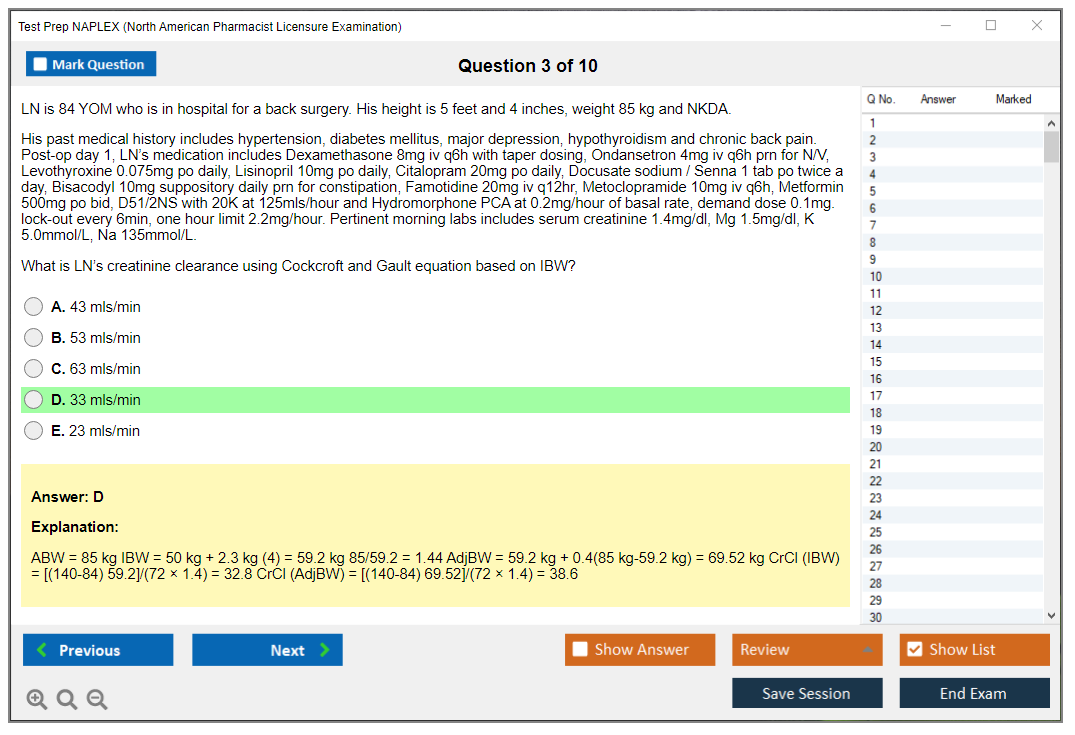
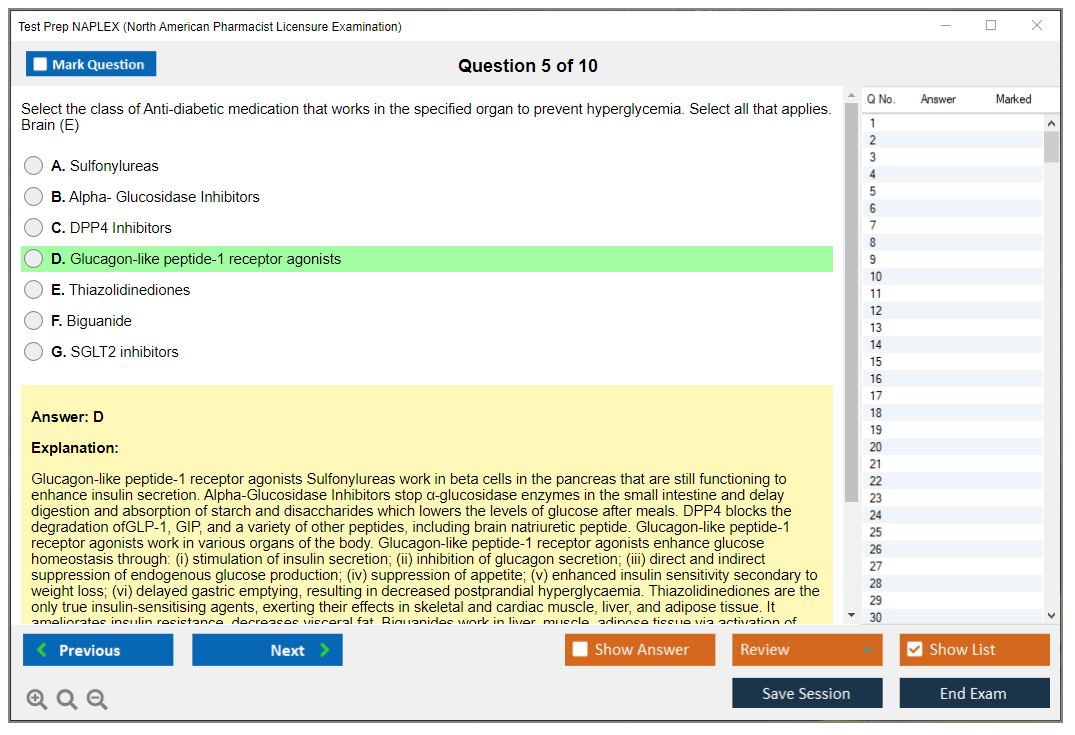
Cardiovascular pharmacotherapy shows up constantly. Hypertension guidelines, heart failure management with guideline-directed medical therapy, anticoagulation decisions between warfarin and DOACs. Endocrine stuff too. Diabetes management across insulin types, GLP-1 agonists, SGLT2 inhibitors, plus monitoring strategies. Infectious diseases questions test antibiotic selection based on spectrum, stewardship principles, HIV therapy. Psychiatric conditions show up too because they cover antidepressants, antipsychotics, seizure medications, and pain management including opioid safety protocols. My cousin actually failed her first attempt because she thought psych meds were low-yield and basically skipped that whole section, which turned out to be a terrible gamble.
Area 2 focuses on ensuring safety and optimizing outcomes through calculations and counseling
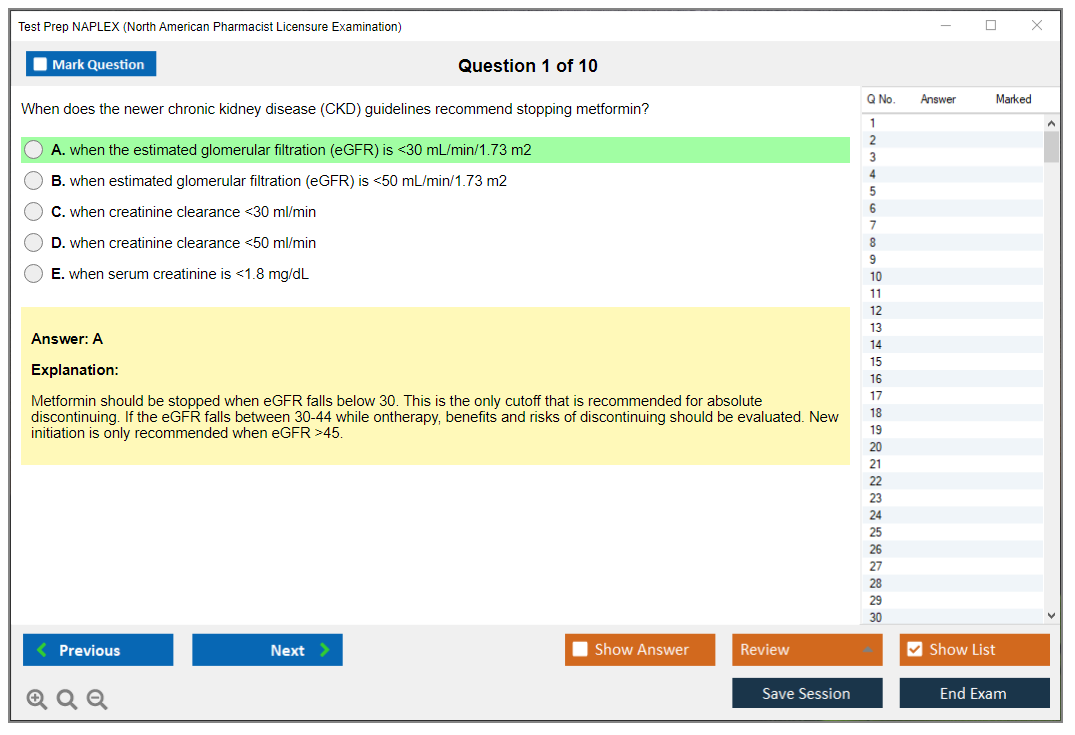
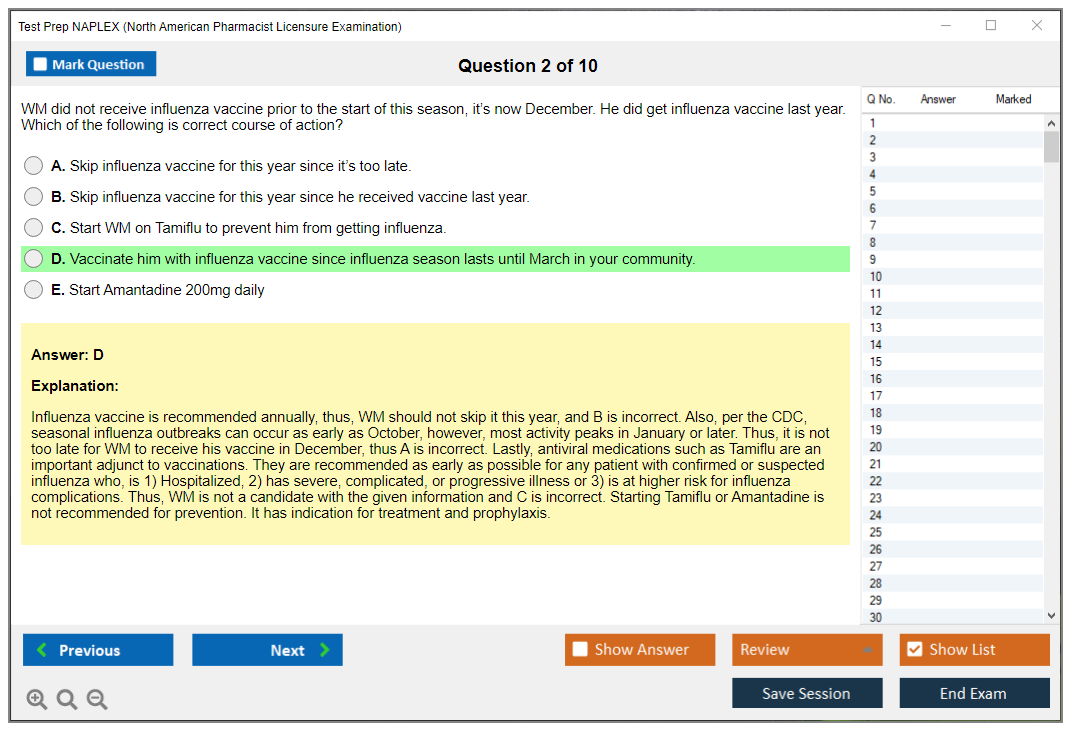
This section takes about 22% of questions but feels way more technical. Pharmaceutical calculations are objective, you either get them right or you do not. Dose adjustments based on renal function, IV drip rates, concentration problems, alligation, milliequivalent conversions. You will calculate creatinine clearance using Cockcroft-Gault, determine ideal body weight versus actual weight for dosing, figure out days supply.
Compounding questions cover both USP 795 (non-sterile) and USP 797 (sterile) requirements, which is similar to what pharmacy technicians study for the PTCE but at a higher clinical level. Beyond-use dating, proper aseptic technique, equipment selection, quality assurance processes. These are straightforward if you know the guidelines.
Medication safety is huge here. High-alert medications like insulin, anticoagulants, and opioids get special attention. REMS programs, look-alike/sound-alike drug pairs, error prevention strategies, adverse event reporting systems. Patient counseling scenarios require you to communicate effectively about administration techniques, expected side effects, adherence strategies without being condescending or overly technical.
Public health and wellness services round out the competency areas
Area 3 is smallest at 11% but do not sleep on it. Immunization questions cover schedules, contraindications, storage requirements, administration techniques. You need to know when someone cannot get a live vaccine, proper refrigeration temps, how to counsel on common side effects.
Disease screening recommendations appear frequently. Diabetes screening criteria, hypertension monitoring, lipid panels, osteoporosis screening in appropriate populations. When do you refer versus manage? Tobacco cessation counseling, weight management interventions, other wellness services pharmacists increasingly provide in expanded practice roles.
How to actually use this blueprint for studying
The official NABP content outline should drive your entire study plan. Spend 65-70% of your time on Area 1 because it is two-thirds of the exam. That is just math. Dedicate specific sessions to calculations since these are high-yield score boosters. They are objective, they are predictable, and practice really improves performance.
Take a diagnostic exam early. Figure out your weak therapeutic areas and allocate extra time there instead of studying what you already know. If you are solid on cardiology but struggle with oncology supportive care, adjust accordingly. The blueprint updates periodically to reflect evolving pharmacy practice, so check NABP's website for the current version before you start.
Similar to how USMLE prep requires focusing on high-yield topics rather than trying to know everything equally, NAPLEX preparation demands strategic allocation. Some people need 2-4 weeks of intensive review, others benefit from 10-12 weeks if there has been a gap since pharmacy school or if foundational knowledge needs rebuilding.
Calculations deserve their own mention again. Percentage strength, ratio strength, alligation problems, days supply determinations. These show up reliably and they are completely learnable through repetition.
NAPLEX Exam Cost and Fees
Look, the pharmacy world basically runs on one hurdle: you've gotta pass NAPLEX to actually practice. State boards use this national competency exam to figure out if you're ready, plain and simple.
Most people take it around graduation. Timing? Yeah, it matters. Not because the test shifts overnight, but honestly, your memory sure does.
NAPLEX tests real pharmacy skills. Not trivia. We're talking patient-specific decisions, safety checks, dosing calculations that seem pretty straightforward until you hit question 87 and your brain's melted into exhaustion.
Also? It's not the MPJE. Different beast entirely.
Seeking U.S. pharmacist licensure? You'll need it in almost every case. International grads face extra hoops first, and some states let you sit early while others don't. That's where paperwork becomes really annoying.
This part's less studying, more bureaucratic approval. The thing is, missing one state board detail is the fastest way to tank your test date.
Education requirements (PharmD/approved program)
You'll need a PharmD from an ACPE-accredited program or approved equivalent pathway for foreign pharmacy graduates. Your school and state board verify everything, but tracking falls on you. Nobody's gonna hold your hand through applications.
State board requirements and NABP registration
You apply through your state board for eligibility AND create an NABP e-Profile. Two systems. Two fees sometimes. Plenty of opportunities to mess up if you're rushing through steps.
ID, authorization to test (ATT), and scheduling basics
Once eligible, you get an ATT (Authorization to Test). That's your green light to schedule with Pearson VUE.
Don't let it expire. Seriously, it happens more than you'd think.
NAPLEX exam objectives follow NABP's blueprint and NAPLEX competency statements. That's your official roadmap for what gets tested, and I mean, it's way more useful than random Reddit threads.
NAPLEX competency statements and major domains
Big categories include patient-centered care, safe and accurate dispensing, public health responsibilities. Questions blend clinical judgment with operational reality, which is why a pure memorization-only NAPLEX study guide feels "okay" but leaves serious gaps.
High-yield topics (patient safety, pharmacotherapy, calculations, compounding)
Patient safety? Everywhere. Pharmacotherapy is relentless. Calculations bleed points, especially when people skip pharmacotherapy calculations review until the final week. Compounding appears too, usually testing whether you can avoid harming someone.
One thing that caught me off guard when I was helping a friend study: the sheer number of "select all that apply" questions that punish you for partial knowledge. You either know the complete picture or you're guessing, and there's no middle ground that feels comfortable.
How the blueprint impacts your study plan
Use the blueprint to allocate daily study time, then pharmacy licensure exam practice questions expose your weak spots. A good plan's honestly boring. Repetition, tracking, fixing errors.
NAPLEX cost and fees
This part nobody wants discussing until they're already paying. NAPLEX exam cost adds up fast in pricey states or if you're forced into retakes because your prep was half-hearted.
NAPLEX exam fee (NABP) and what it covers
The current NAPLEX exam fee charged by NABP is $575, but verify current year pricing because fees adjust periodically and they do increase from time to time, just so you know. You pay NABP directly during registration inside the NABP e-Profile system. Not your school, not Pearson VUE.
That $575 covers one complete exam attempt, including scoring, score transmission to the state board(s) you designate, and access to your online score report. Payment's due at registration and must be made by credit card, debit card, or electronic check. One more thing people constantly miss: the fee becomes non-refundable once your ATT's been issued, so if you're uncertain about readiness, decide that before clicking pay.
Additional costs (state board fees, rescheduling, travel)
State board fees are separate and wildly inconsistent. Usually $50 to $400 or more depending on jurisdiction, plus whatever processing fees that board randomly adds. Background checks are common, often $30 to $100, and fingerprinting can run $40 to $75. Some states also require a state law exam with variable fees, so budget for it even if your classmates in another state didn't pay.
MPJE's another line item. If your state requires it, MPJE costs $225, and yeah, MPJE vs NAPLEX differences matter because you can't study for law like it's pharmacotherapy.
Rescheduling can sting. Pearson VUE charges $60 if you reschedule with less than 3 business days' notice. No fee if you move it earlier. Travel's the sneaky cost: if the nearest test center is far, you might need a hotel, transportation, meals, parking. That can easily rival the exam fee if you're unlucky with locations. If you're applying in multiple states, some candidates also budget for expedited score transfer fees, which isn't "required" but can speed timelines when you're chasing job offers.
Retake fees and waiting periods (state-dependent)
Fail? You pay the full $575 again for every attempt.
No discount. Not gonna lie, that alone argues for buying decent NAPLEX study materials upfront, like $200 to $500 worth, because a single retake costs more than a whole prep stack.
Retake policies depend on your state board. Some allow quick retesting, others impose waiting periods like 30 days (many states), 45 days, 60 days, or even 90 days between attempts, and you'll need a new ATT for each retake. Some states also cap total attempts, commonly 3 to 5, before requiring remediation or additional education, and a few demand remedial coursework or written study plans after multiple failures. If you're worried about your baseline, budget for 2 to 3 attempts on paper, then plan like you only want to pay once.
If you want structured practice without spending a fortune, start with a targeted question set like the NAPLEX Practice Exam Questions Pack and use it to drive your weak-area study, then add a full NAPLEX practice test later when your accuracy stabilizes. I've seen people burn weeks rereading a NAPLEX study guide while ignoring performance data, and then they're shocked by NAPLEX exam difficulty on test day.
NAPLEX passing score and scoring explained
NAPLEX uses scaled scoring. The NAPLEX passing score is 75. Your raw correct count isn't shown the way school exams do it, which is why chasing "percent correct" on random quizzes can mess with your head.
Score reporting typically shows up after processing, viewable online. Don't pass? Your next steps depend on your board's retake rules, and you'll be back to paying fees and waiting out the clock.
FAQ (Quick answers)
How much does the NAPLEX cost?
$575 paid to NABP, plus state fees and extras like MPJE, fingerprints, travel.
What is a passing score on the NAPLEX?
75 (scaled).
How hard is the NAPLEX compared to pharmacy school exams?
Harder in a different way: longer, more applied, more fatigue-based.
What are the best study materials for NAPLEX prep?
A solid question bank, reliable NAPLEX study guide, guidelines, repeated calculations drills. The NAPLEX Practice Exam Questions Pack is a cheap way to start pressure-testing knowledge.
How many practice tests should I take before the NAPLEX?
Enough to see consistent improvement and stable timing, usually 2 to 4 full runs plus focused sets. If you're behind, do fewer full tests and more targeted review with something like the NAPLEX Practice Exam Questions Pack to stop repeating the same misses.
The scaled score system and what 75 actually means
The NAPLEX doesn't work like your pharmacy school exams where you could calculate a percentage and know exactly where you stood. The exam uses a scaled score ranging from 0 to 150, with the passing score set at 75. But that 75? It doesn't mean you got 75% of questions correct.
The scaled scoring system converts your raw score (basically the number of questions you answered correctly) to a standardized scale that accounts for difficulty variations between different questions. Since the NAPLEX uses computer-adaptive testing, each candidate gets different questions based on how they're performing. If you're crushing it, the algorithm serves up harder questions. Struggling? You'll see easier ones.
This CAT format means we can't just count correct answers and call it a day. Scaling creates fairness across all test forms, so someone who happened to get slightly easier questions doesn't have an unfair advantage over someone who got brutally difficult ones.
You can't calculate your own score during the exam. Honestly, trying to guess whether you're passing while you're taking it'll just mess with your head. Only the final scaled score matters for pass/fail determination, and there's no published "percentage correct" equivalent because of the adaptive algorithm working behind the scenes.
The passing standard of 75 represents minimum competency level determined by NABP through standard-setting studies involving pharmacy practitioners and educators. They basically gathered experts to decide what level of knowledge a newly licensed pharmacist needs to practice safely. All 50 states, DC, and U.S. territories use this same passing standard. It's a universal requirement, which actually makes things simpler.
How the scoring actually works question by question
Here's something that trips people up constantly: partial credit isn't awarded. Each question's scored as correct or incorrect only. No gray area whatsoever.
The exam's got 250 total questions, but only 225 count toward your final score. The other 25? They're pretest items scattered throughout the exam, used for future exam development. Candidates can't identify which questions are pretest versus scored, so you've gotta treat every single question like it matters. That weird question about some obscure drug interaction could be the one that pushes you over the line.
Similar to how the MCAT-Test uses experimental sections that don't count toward your score, NAPLEX pretest items help maintain exam quality without penalizing test-takers. You must answer all questions since pretest items aren't marked differently.
I remember talking to a friend who spent 10 minutes on what turned out to be a pretest question. Tanked his timing for the rest of that section. You can't know which ones matter, which is sort of maddening when you think about it.
Getting your score and understanding what it tells you
Unofficial pass/fail results are available online through your NABP e-Profile typically within 7 business days after testing. Official score reports with your numerical scaled score get sent to you and your designated state boards within 7 to 10 business days.
Score reports include your scaled score, pass/fail status, and performance feedback by competency area showing whether you performed above, near, or below expectations in different domains. This competency area feedback helps failing candidates identify weak content areas for targeted retake preparation. Super useful if you need another shot at it.
What you won't see? Raw scores. Percentage correct. Individual question feedback. The NABP keeps that locked down tight.
Candidates who pass receive scores of 75 to 150, while failing candidates receive scores of 0 to 74. There's no honors or distinction for high scores, which honestly takes some pressure off. Passing's passing regardless of whether you scored 76 or 145, though I've got mixed feelings about whether that's truly fair since some people really do demonstrate exceptional mastery.
Scores are automatically transmitted to the state board you designated during registration. Need to transfer scores to additional states? That requires separate requests and fees. Score portability's pretty good though. NAPLEX scores are valid indefinitely for initial licensure, though some states have time limits between passing and actually applying for your license.
When you don't pass and what comes next
First thing after failing: review your score report competency feedback to identify weak areas. That breakdown by competency area? It's gold for figuring out where to focus.
You need to create a targeted study plan focusing on those "below expectation" competency areas before retaking. Resources like the NAPLEX Practice Exam Questions Pack at $36.99 can help you drill specific content areas where you struggled. Candidates must apply to their state board for permission to retake and get a new authorization to test.
State-specific waiting periods range from 30 to 90 days between attempts. Check your state board requirements because they vary wildly. It's frustrating how inconsistent the rules are from state to state. Some states require proof of additional study or remedial coursework after a second or third failure.
Each retake requires the full $575 exam fee payment and new registration through NABP. Most states limit total attempts (typically 3 to 5 within specific timeframes) before requiring additional education or remediation.
If you've failed multiple times, consider formal review courses, tutoring, or additional clinical experience before your next attempt. Unlike standardized tests like the GRE-Test or GMAT-Test where retaking's more common, pharmacy boards take multiple NAPLEX failures seriously.
Here's the emotional reality: failing isn't uncommon, with approximately 10 to 15% first-time failure rate. Many successful pharmacists needed multiple attempts. The NAPLEX Practice Exam Questions Pack helps you gauge readiness before committing to another $575 attempt. Don't rush the retake just to get it over with. That's how people end up burning through their allowed attempts.
How Difficult Is theNAPLEX?
NAPLEX in plain terms
The North American Pharmacist Licensure Examination is the big clinical gatekeeper for pharmacists in the US. It tests whether you can take patient info, make safe medication decisions, and handle the math that keeps people from getting hurt. Not cute trivia.
What the test actually looks like
You'll sit for about 6 hours and answer 250 questions. That's forever to stay sharp, and honestly the length alone makes the NAPLEX exam difficulty feel higher than it might be on paper. Breaks exist, but fatigue still stacks up. Your brain starts doing that thing where you reread the same line three times. Like, you know you're reading words, but they're just not landing.
why people walk out thinking it was brutal
Difficulty is subjective. I mean, it depends on how you prepared, how strong your rotations were, whether you were working full time, and how long it's been since graduation. Someone fresh off an acute care APPE with constant dosing adjustments might feel fine. Someone who's been away from clinical decision-making for a year can feel like the test is written in a different language.
The computer-adaptive vibe messes with people too. NAPLEX isn't fully adaptive in the "every single question changes your path" way like some exams, but it does adjust difficulty based on performance. When you keep getting harder questions after "good" answers, it can feel like you're failing the whole time. Zero confidence boost. Just uncertainty hanging over every click.
Another big one: the question style is application-heavy. Pharmacy school exams can reward recall, like "what's the MOA" or "what adverse effect," but the NAPLEX likes "here's a patient with five problems, eight meds, and labs, now pick what you'd do." Extra info is everywhere on purpose, like real practice, so you have to filter what matters and ignore the noise. That sounds simple until you're 4 hours in and your eyes are crossing.
Multi-step reasoning is the sneaky killer. One question can ask you to assess the patient, spot the medication-related problem, choose an intervention, and predict what happens next, all in one go, while also noticing the potassium is low and the creatinine clearance is worse than it looks. Time pressure makes that harder. You get roughly 1.5 minutes per question including reading long cases that sometimes feel deliberately bloated with irrelevant family history or social details you'll never need.
I once spent 90 seconds on a vignette about a patient's weekend fishing trip before realizing it had nothing to do with his anticoagulation adjustment. Still mad about it.
Math adds stress too. Calculation questions demand accuracy under pressure, and you don't get your personal calculator. Only a basic on-screen one. If you're used to flying through dosing and compounding math on paper, the tool change alone can slow you down. The thing is, it's not even a fancy calculator, just basic functions, which somehow makes simple operations feel clunky.
Breadth is another reason candidates struggle. NAPLEX covers basically all therapeutic areas, so you can't "strategically skip" entire disease states and still feel safe. Even if you hate ID or oncology, it's still showing up. Probably multiple times. With weird drug names you saw once in P2 year.
Also, "select all that apply" questions. No partial credit. That format punishes second-guessing, and test anxiety makes second-guessing your default setting, even when your knowledge base is actually fine. You'll sit there thinking "is it three answers or four?" and spiral for 30 seconds you don't have.
the two sections people complain about most
Calculations and clinical application. Not gonna lie, that tracks with what I see from candidates using Test Prep NAPLEX plans and any decent NAPLEX study guide.
Pharmaceutical calculations are high-difficulty because they're precise and unforgiving. You can know the concept and still miss a unit conversion, forget to round properly, or misread the question. Common pain points include IV drip rates, compounding concentrations, pediatric weight-based dosing, renal dose adjustments, and alligation. The annoying part? You usually know the formula. But time pressure makes dumb mistakes more likely, especially if you're toggling the on-screen calculator and trying not to lose your place in the stem. I've watched people nail a practice problem in 30 seconds, then freeze on test day because the wording was slightly different.
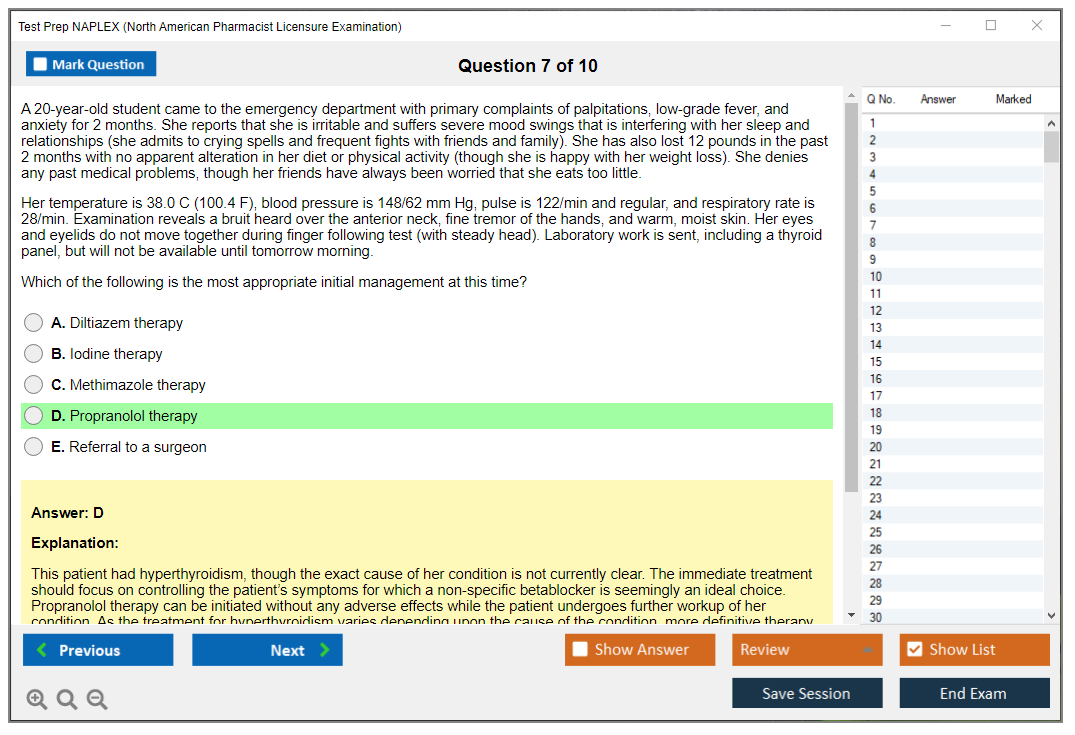
Clinical application is the other monster because it forces integration. Pharmacology plus pathophysiology plus pharmacokinetics plus patient-specific factors like age, pregnancy, organ function, allergies, and adherence, all at once in a messy vignette that mirrors actual hospital chaos. Some questions basically test whether you can pick a drug for a complex patient with multiple comorbidities, while avoiding interactions and contraindications, and still hitting guideline goals. Strong students get tripped up here because there isn't always one "school answer." There's the "best" answer for that specific patient, which can feel subjective even though it's not.
Therapeutic monitoring shows up constantly. Goal ranges, timing of levels, and what to do with the result. Think vancomycin, warfarin and INR management, lithium, antiepileptics. Counseling scenarios can be weirdly hard because you're choosing the most appropriate communication approach, not just listing side effects. Soft skills, but tested like clinical judgment, which feels unfair but also kinda real?
Compounding can be rough. Sterile and non-sterile prep, beyond-use dating, and USP chapters, plus practical workflow decisions nobody actually taught you in a structured way. Medication safety questions hit error prevention strategies, high-alert meds, and REMS program basics. And yeah, there are always less commonly taught areas that pop up and make you mad. Obscure antidotes. Oddball compatibility details. Operational safety policies you only half remember from rotation.
how does it compare to the mpje
The MPJE vs NAPLEX differences are pretty straightforward. MPJE is law and policy, lots of "what is allowed," and your state-specific rules matter. NAPLEX is clinical and math heavy, and it feels more like being on rotation with a preceptor who keeps asking "okay, but what would you do next?" while staring at you expectantly.
quick money and scoring stuff people ask about
The NAPLEX exam cost includes the NABP fee, and then you may have state board fees on top. Plus possible rescheduling or travel costs depending on your test center. Not cheap. Budget accordingly.
The NAPLEX passing score is reported as a scaled result, and "passing" is the threshold your state recognizes. You don't need perfection. You need consistent competence across the NAPLEX exam objectives. That's it.
how to make the difficulty feel manageable
Use NAPLEX study materials that match the exam style. Lots of pharmacy licensure exam practice questions, a focused pharmacotherapy calculations review, and at least one full NAPLEX practice test to train endurance because sitting that long is its own skill. The key is review quality, not volume. Track why you missed questions, fix the gap, then retest that exact concept until it sticks.
eligibility basics people forget
Who can even sit for it
Your NAPLEX prerequisites usually mean a PharmD from an accredited or approved program, plus state board requirements, NABP registration, and an authorization to test before scheduling. Paperwork mistakes delay everything. Dumb, but real, and I've seen people miss their test window over a missing signature.
last reality check
"How difficult is the NAPLEX?" It's hard in the way real pharmacy is hard. Messy info, time pressure, and consequences. If you prep with realistic question banks, practice endurance, and treat calculations like a daily skill instead of a one-week cram, the difficulty drops fast, even if the test still feels uncomfortable the whole time. You'll survive it. Most people do.
Conclusion
Getting real about your NAPLEX prep timeline
Look, I've seen too many pharmacy grads underestimate this exam. The NAPLEX isn't something you can cram for over a long weekend like some pharmacy school finals. It just doesn't work that way. Your Test Prep NAPLEX strategy needs to be deliberate, especially if you've been out of school for a minute or had rotations that didn't hit every therapeutic area hard.
The biggest mistake? Treating NAPLEX study materials like a checklist instead of actually learning from your mistakes. You can read through five different NAPLEX study guides, but if you're not tracking why you missed questions on pharmacotherapy calculations or misapplied NAPLEX competency statements in clinical scenarios, you're just spinning your wheels. Really sit with those explanations. The exam doesn't just test recall. It tests whether you can apply guidelines in messy real-world contexts where patient safety depends on your clinical judgment, and that's a completely different skill set.
Your NAPLEX passing score depends on scaled performance across all domains. That makes practice testing more critical than it was in school, which honestly caught me off guard when I first started prepping. One diagnostic North American Pharmacist Licensure Examination prep test early in your timeline shows you where the gaps are. Do this first. Then you need at least three to four full-length NAPLEX practice tests under timed conditions before test day, spacing them out so you can actually address weak areas between attempts. Don't just chase volume. Chase understanding. Also, and this is something nobody tells you, if you're working retail or hospital shifts while studying, you'll need to block off actual rest days. I tried powering through once and bombed a practice test because my brain was fried from back-to-back closing shifts.
Final recommendations for exam success
The NAPLEX exam cost isn't cheap. Neither is your time. Factor in the NAPLEX exam difficulty when you're building your study schedule. This isn't MPJE, where you're memorizing state-specific law. This tests whether you can actually practice safely as a pharmacist on day one, which is a whole different level of pressure. If you're wondering what the best study materials for NAPLEX prep actually are, start with pharmacy licensure exam practice questions that mirror the adaptive format and clinical depth you'll face.
Here's what I'd do: grab the NAPLEX Practice Exam Questions Pack and use it as your baseline diagnostic, then as your final confidence check two weeks before your exam date. The questions are built around actual NAPLEX exam objectives, hitting those high-yield calculation scenarios and patient case applications that trip people up. These scenarios catch even strong students. You've already invested years in your PharmD, so invest in materials that actually prepare you for the format and rigor of test day, not just generic pharmacy review content.
You've got this. But prepare like it matters, because it does.